Make an Appointment
So you’ve ruptured your Anterior Cruciate Ligament (ACL)? Chances are you did it skiing or playing soccer or oztag or in some other activity that challenged the stability of your knee. If you want to continue performing these activities, chances are you will need to have surgery to repair / replace your ACL. There are many graft options now available and the aim of this article is to arm you with some information to help you make your decision. It is important to realise that some graft options have been along longer than others and hence have more long-term data associated with them.

More Articles Related to Surgery

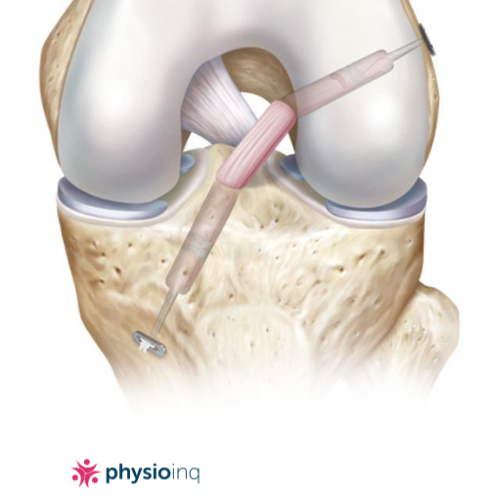
The aim of ACL reconstruction surgery is to restore the passive internal stability of the knee. In specific terms it is to prevent anterior (forwards) translation (movement) of the tibial relative to the femur as well as providing stability on the rotational plane. It would make sense that the graft choice should have similar properties to a normal ACL.
There are three commonly used graft types, one that is less commonly used and one that is still in the experimental stage. We will cover all of these to some degree in this article.
The three most commonly used graft types are:
- Patella Tendon Graft
- Hamstring Tendon Graft
- Synthetic / LARS graft
A less commonly used graft is the allograft. An allograft is a tendon that is harvested from a cadaver.
A graft type that is still in the experimental stages is often referred to as the 'blood bridge'.
To date, no graft types have been able to reproduce the anatomy and function of the original ACL. By far the Patella tendon and Hamstring Tendon graft are the most popular choices of surgeons today.
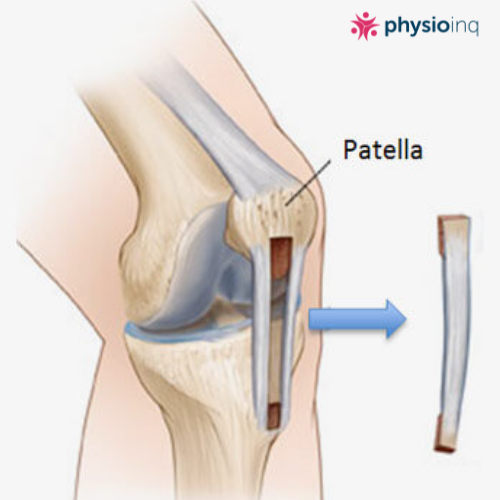
Patella Tendon Graft
More Articles Related to Sport



This graft is taken from your Patella tendon. The middle third of the tendon is removed with a piece of bone from both the patella and the tibia still attached. These small pieces of bone on each end are inserted into tunnels on both the femur and tibia as anchor points during the reconstruction.
Pros:
- Earlier bone to bone healing. This is thought to be stronger and resistant to earlier aggressive rehabilitation following surgery.
- Decreased anterior knee laxity.
- No hamstring graft site.
Cons:
- Higher chance of anterior knee pain, in particular if the patients job or sports involves kneeling.
- Greater chance of knee extension strength loss.
- Greater chance of post-operative complications such as patella tendon rupture or patella tendinitis.
- Larger incision.
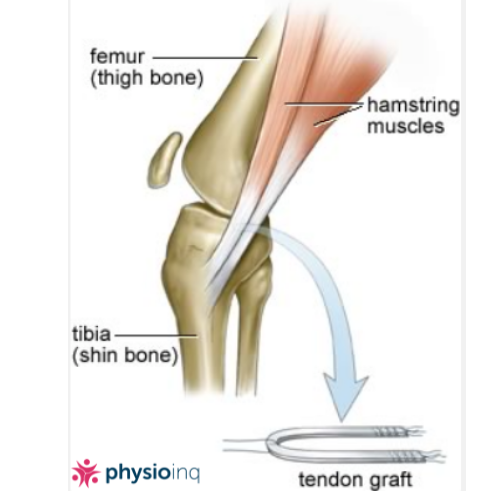
Hamstring Tendon Graft
More Articles Related to Mobile Physiotherapy



Of late, the hamstring tendon has become a very popular graft choice. The graft is harvested from Gracilis and Semitendinosis tendons and then doubled up to make four strands. This is a bone to tendon graft (no bone is grafted with the tendons) where the tendons are fixated within a bony tunnel. This type of graft needs solid healing within the bone tunnel as quickly as possible after surgery.
Pros:
- Larger graft diameter, which is thought to make is stronger.
- Much lower risk of anterior knee pain.
- Smaller incision.
- Less pain in the immediate post-operative period.
- No Patella Tendon graft site.
Cons
- Longer recovery time is required. The bone to tendon graft does not heal as quickly as the bone to bone graft.
- Greater chance of knee flexion strength loss
- May cause an imbalance of the medial hamstrings to the lateral hamstrings causing knee pain and increased chance of hamstring injuries.
- Often associated with bruising to the posterior knee.
For more on rehabilitating hamstring injuries go to /blog/hamstringinjuries_treat_strategies
Synthetic/LARS Graft
This graft is an artificial graft that is made of synthetic material. It has become popular in the domain of elite sports in the last decade, although has not been used long enough or extensively enough for good long-term data to be established and analysed.
Pros:
- No graft site that needs to recover post-surgery.
- Less incisions.
- Able to be used when multiple ACL reconstructions have been performed and hence other graft sites have been exhausted.
Cons:
- Not enough long-term data on the efficacy of this graft type.
- Some preliminary data shows a possible increased risk of knee Osteoarthritis when compared to other graft types.
- Potential for rejection.
Allograft
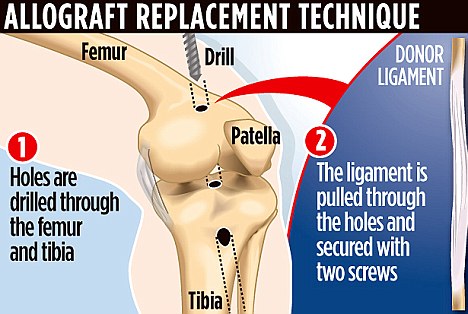
A less commonly used graft is the allograft. An allograft is a tendon that us harvested from a cadaver.
Pros:
- No graft site that needs to recovery post-surgery.
- Less incisions
- Able to be used when multiple ACL reconstructions have been performed and hence other graft sites have been exhausted
Cons:
- Not enough long term data on the efficacy of this graft type.
- Potential for rejection.
Blood Bridge
A graft type that is still in the experimental stages is often referred to as the ‘blood bridge’. This refers to a surgical procedure where instead of replacing the ruptured ACL with a graft, a small sponge that is soaked in the patient’s own blood is placed in between the two ends of the ruptured ACL providing a ‘bridge’ for the two ends to grow across and re-attach. As mentioned, this surgical option is still in the trial phases and is not currently used routinely.
In a recent study, 10 patients underwent the procedure. Impressively, on follow-up, all 10 ACLs had grown across and ‘blood bridge’ and re-attached. This is only the early stage but it is promising. We are yet to hear the long-term data and results. Although all 10 re-attached, the important information is how strong is the re-attached ACL and has it re-attached at an appropriate length to make it viable to perform its function?
While there are many graft options available, there still does not appear to be a gold standard or a consensus on which is best. Most graft choices have advantages and disadvantages. Most graft choices will affect pain levels and how aggressively rehabilitation can commence; hence these factors should be discussed with the orthopaedic surgeon.
If the thought of creating a prehab program yourself sounds overwhelming, we can help! We have a team of Mobile Physio’s and Exercise Physiologists across Australia ready to assess and educate you on your options with your ACL injury. Contact us by phone at 1300 731 733 or find a location nearest to you to get started!
Date Published: Wednesday, February 6, 2019
More Articles Related to Surgery


More Articles Related to Sport
More Articles Related to Knee




Locate a Mobile Physiotherapy
Service Near me
Get the experience & convinence you deserve to support your or a loved one's allied health needs.
Our Mobile Physiotherapy team are currently serving & taking appointments in the following states and regions in Australia:
New South Wales
- Blacktown
- Blue Mountains
- Campbelltown And Macarthur
- Canterbury-Bankstown
- Eastern Suburbs Sydney
- Georges River
- Hawkesbury
- Inner East Sydney
- Inner West Sydney
- Lake Macquarie
- Lower North Shore
- Newcastle
- Northern Beaches
- North Sydney
- Parramatta
- Penrith
- Southern Highlands
- South West Sydney
- Sutherland Shire
- Sydney CBD
- The Hills Shire
- Upper North Shore
- Waverley
- Wollongong
Tasmania
Victoria
Need to get into direct contact with ur Client Services team? We're all ears. Call our team directly on 1300 731 733
