Why are Shoulder Injuries Common in Overhead Sports?
Our shoulder joints are the most mobile joints in the human body. Yet, there is a tradeoff for all this mobility in the form of instability leading to high numbers of shoulder injuries in sports.
More Articles Related to Sport

The least stable position for your shoulder to be in is having your arm raised 90 degrees to the side with your elbow bent 90 degrees with your hand facing forward. In simplistic terms;
“Your shoulder is at its weakest when doing overhead sport like swimming, rock climbing, or any type of throwing.”
Overhead sport can lead to both traumatic and atraumatic overuse injuries to the shoulder.
- Traumatic injuries like a shoulder dislocation often occur in competition settings from things like hard landings and tackles.
- Atraumatic injuries like tears causing sports injury shoulder pain often occurring in a training setting and are related to high repetition of the same movements or heavy loads.
Common Sports Shoulder Injuries
These are the most common sports-related shoulder injuries that are caused by playing overhead sports.
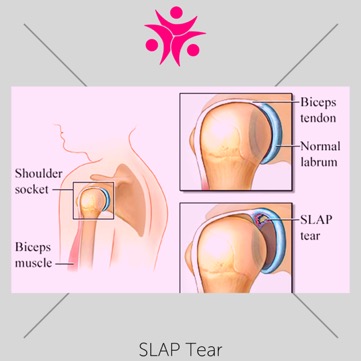
SLAP Tear
Surrounding your shoulder socket is a ring of cartilage (labrum). A SLAP tear is a rip in this cartilage. It develops from repetitive overhead movements over time.
Symptoms of a SLAP tear include:
- A decrease in athletic ability when it comes to power in overhead throws and feeling like your shoulder could “pop out”
- Pain caused by certain movements like swinging a tennis racket
- Limited range of motion overhead
- A deep, achy pain that you’re unable to pinpoint
- Clicking, grinding, locking, or popping sensations in your shoulder
More Articles Related to Shoulder



Shoulder Instability
Common in contact sports, like rugby or hockey, and in those that require repetitive movement, like cricket, shoulder instability is a common injury among athletes.
It occurs when the ligaments, muscles, and tendons of your shoulder are destabilised. This results in the round part of your upper arm bone (humeral head) either dislocating (coming out completely) or subluxation (partially coming out) from the shoulder socket.
Dislocation causes a sudden and severe onset of pain while subluxation is accompanied by short bursts of pain.
Symptoms also include:
- Arm weakness
- Lack of movement
- Swelling
- Bruising
Rotator Cuff Injury
Rotator cuff injuries are common in overhead sport, they’re painful, and are characterised by weakness in the shoulder, reduced range of motion, and stiffness.
The pain of a rotator cuff often comes in three forms:
- While sleeping if you sleep on the side with the shoulder injury
- In motion, especially during overhead movements
- Throughout your entire arm
- Similar to how SLAP tears feel with an ache in the shoulder
Sport-Specific Injuries
In the next section, we will deep dive into the most common overhead and shoulder injuries for each sport.
Baseball
"The repetitive nature of pitching in baseball puts players at risk for shoulder instability due to microtrauma and microinstability (31) (Table). Reinold et al. (32) found a 5-degree increase in external rotation among professional baseball pitchers at the end of the season compared with the beginning of the season. This progressive loss of internal rotation and increase in external rotation can theoretically cause attenuation of the anterior capsular tissues and lead to microinstability (9). Injuries to the labrum, both anterior-inferior (Bankart lesion), and superior (SLAP lesion), are common among baseball players, especially pitchers. Specifically, SLAP tears may be related to GIRD (33). Burkhart et al. reported on a series of 124 baseball pitchers with type II SLAP lesions (detachment of biceps anchor) and reported that the mean GIRD was 53 degrees in the overall patient cohort, with mean GIRD of 33 degrees in those with type II SLAP lesions (31)." - Taken from DeFroda, Steven F. and their article on Shoulder Instability in the Overhead Athlete
Tennis
"The overhand tennis serve puts tennis players at risk of developing shoulder instability in a mechanism similar to that of overhead throwers (35). For this reason, tennis players also are susceptible to GIRD and SLAP tears, which may alter shoulder kinematics or lead to subtle instability (35). Lädermann et al. (36) sought to examine glenohumeral instability and impingement patterns during tennis movements by determining the type and frequency of impingement as well as the amount of shoulder subluxation. Ten former asymptomatic professional tennis players were recruited and evaluated for internal and external impingement as well as glenohumeral instability using optical motion capture (OMC) kinematics testing, MRI, and clinical exam. All players had a competent rotator cuff clinically, while MRI revealed cuff lesions in six of the subjects (encompassing three interstitial tears of the supraspinatus and eight partial articular supraspinatus tendon avulsions [PASTA] lesions). Labral tears were evident in five of the athletes (two posterior, two inferior, and two posterosuperior lesions). There was no evidence of Bennett or Bankart lesions. OMC testing revealed anterosuperior impingement in two athletes during their forehand. Four athletes were found to have anterior and lateral subacromial impingement and seven were found to have posterosuperior impingement during the late cocking phase of serving (36). The authors recommended utilizing a more compact serve motion to minimize impingement that can occur along with instability." - Taken from DeFroda, Steven F. and their article on Shoulder Instability in the Overhead Athlete

More Articles Related to Mobile Exercise Physiology



Volleyball
"Volleyball produces different kinematics than throwing; however, this sport also involves repetitive overhead activity, which can stress the glenohumeral joint beyond its physiologic limits. However, because the movements required for serving, spiking, and setting in volleyball are slightly different than overhead throwing, athletes will manifest their instability in a different form, typically as multidirectional instability (MDI) (35). It can be difficult to predict what patients are at risk for further injury, or progression to frank dislocation. Therefore, patients should be closely monitored with regards to their symptoms and performance, and be removed from play if symptoms persist. Kinetic forces about the shoulder are the greatest during spiking, and those athletes who frequently perform this activity both in games and practice should be monitored for signs of overuse (37). Over time, the repetitive motion associated with the volleyball serve can lead to chronic attenuation of the capsular tissue, resulting in apprehension during overhead activity with the arm in forward elevation and abduction or even activities of daily living. Patients with redundant capsular tissue may be candidates for a capsular shift, remplissage, or both. Jones et al. reported on the outcomes of 20 overhead athletes (six baseball, four swimming, three softball, three volleyball, three tennis, and one water polo) who underwent arthroscopic capsular plication (12 with suture, eight with suture anchors) for debilitating shoulder pain secondary to symptoms of anterior instability without evidence of frank dislocation (38). At a mean follow-up of 3.6 years, 18 (90%) patients returned to play, with 17 (85%) at their preinjury level of play. The two patients who failed to return to play had concomitant rotator cuff injury and continued pain postoperatively (38).
While HAGL lesions have been described in baseball athletes, this injury also may be seen in competitive volleyball players, as the extreme abduction and external rotation obtained during a volleyball serve can approach that experienced during a baseball pitch. However, the presurgical diagnosis of HAGL lesion as a cause for anterior shoulder instability can be difficult. Taljanovic et al. (39) examined a series of four female collegiate volleyball players with chronic activity-related pain and inferior capsular laxity and/or instability in their dominant shoulders. The authors were specifically interested in the presence of HAGL lesions as evidenced by MR arthrogram and arthroscopy. All four patients were found to have HAGL lesions. Three also were found to have articular sided partial-thickness rotator cuff tears and three were found to have labral tears, which were repaired with suture anchors (one SLAP, one midline posterior labral avulsion tear, and one chronic appearing anterior inferior avulsion tear). The authors emphasised that repetitive microtrauma from overhead hitting in volleyball can lead to inferior capsular laxity and subsequent HAGL lesions (39). Physicians should keep this injury in mind when evaluating volleyball players." Taken from DeFroda, Steven F. and their article on Shoulder Instability in the Overhead Athlete
Swimming
"Similar to volleyball, swimmers also are subject to MDI and generalised ligamentous laxity (40). “Swimmer’s shoulder” is a term used to encompass a wide array of pathology (subacromial impingement, biceps or rotator cuff tendonitis, or just generalised shoulder pain), which effects this patient population (41). Tate et al. investigated risk factors for shoulder pain and disability, although not necessarily instability, across the career of swimmers by examining 236 swimmers ages 8–77 (41). The pain profile and symptomology varied with age and exposure. Patients younger than 12 years primarily had pain, whereas older patients more commonly complained of disability and inability to use their shoulders; with high school athletes being the most symptomatic (41). The factors found to contribute most to shoulder pain were greater swimming exposure, history of traumatic injury (common in swimmers who also played water polo), and those who experienced feelings of subjective instability (41). This study underlies the importance of educating swimmers about the risk factors for developing long-term disability in general, so that issues such as recurrent instability, which has been shown to contribute to shoulder pain later in life, may be addressed sooner rather than later." Taken from DeFroda, Steven F. and their article on Shoulder Instability in the Overhead Athlete

Ways to Prevent Shoulder Injuries When Doing Overhead Sports
One of the main things we can do to prevent shoulder injuries in sports is to properly manage your training schedule and pay attention to how heavy a load you’re carrying. This looks different for every overhead sport, but especially leading up to a game season/event, it’s important to check in on what you can handle.
The next thing you’ll want to do, and what physiotherapy can help you with, is to strengthen your rotator cuff. If you’re playing an overhead sport, you’ll need an extra strong shoulder joint.
- Lie on your stomach. Extend one arm with your elbow bent 90 degrees, hand toward the floor. Keep your elbow bent and slowly raise your hand until it’s in line with your shoulder. Lower your hand slowly and repeat ten times. Switch arms.
- Stand with your arms extended slightly behind you, thumbs down. Raise your arms, keeping them straight. Lower slowly. Repeat ten times.
Before you do anything, make an appointment with one of our Physio Inq clinicians or your local physiotherapist for personalised shoulder exercises to help strength the joint and prevent ongoing and referring injuries.
How to Treat Shoulder Injuries from Overhead Sports
First and foremost, treatment for a shoulder injury starts with rest. Your movement will be limited and painful already but it’s truly best not to push through and keep using your shoulder. Unfortunately, if you have a shoulder injury, the first step is rest.
If you have a dislocated shoulder, treatment can’t really begin until reduction takes place. “Reduction” is a medical term for shifting the joint back into place. This can be an incredibly painful procedure and sometimes requires a sedative.
In addition to rest, ice, and anti-inflammatory/pain-relief medications, physiotherapy is an incredibly important aspect of the treatment plan for overhead sport shoulder injuries. Since each person’s injury and physicality is unique to them, it’s important that your rehabilitation plan is tailored to you.
Here at Physio Inq, our certified mobile physiotherapists and clinic physiotherapists can crete individualised plans built for your unique needs. We work with athletes and exercise goers all throughout Australia and with our mobile services, our physiotherapists can even come to you. If you’re suffering from a debilitating shoulder injury, give us a call. We’re eager to help get you back on track.
Date Published: Monday, June 22, 2020
Date Modified: Tuesday, July 2, 2024
More Articles Related to Sport

More Articles Related to Shoulder


Locate a Mobile Exercise Physiology
Service Near me
Get the experience & convinence you deserve to support your or a loved one's allied health needs.
Our Mobile Exercise Physiology team are currently serving & taking appointments in the following states and regions in Australia:
New South Wales
- Blacktown
- Blue Mountains
- Campbelltown And Macarthur
- Canterbury-Bankstown
- Central Coast
- Eastern Suburbs Sydney
- Georges River
- Hawkesbury
- Inner East Sydney
- Inner West Sydney
- Lower North Shore
- Newcastle
- Northern Beaches
- North Sydney
- Parramatta
- Penrith
- South West Sydney
- Sutherland Shire
- Sydney CBD
- The Hills Shire
- Upper North Shore
- Waverley
- Wollongong
Tasmania
Victoria
Need to get into direct contact with ur Client Services team? We're all ears. Call our team directly on 1300 731 733
